Full Pay Restoration in England: A Strategic Discussion
The Broad Left in the BMA is a group of union activists and local organisers across the four nations and the various branches of practice, unified by a belief in rank-and-file organisation, transparency and democracy in the BMA, and protection of the NHS.
On the 1st of August, the Broad Left held a meeting to discuss the first 2024 English Resident Doctor Pay Offer presented to the membership by the Resident Doctors Committee (RDC, formerly Junior Doctor Committee (JDC)). At this meeting, there were diverse opinions within Broad Left on whether members should accept or reject the offer based on the best strategy to achieve Full Pay Restoration.
This article outlines the key points in the debate, written by members on either side, and we hope that it will be helpful and informative to resident doctors and the wider labour movement.
Sections
The offer
Where members of Broad Left are in agreement
Where members of Broad Left have varying views
The Reasons to Vote Reject.
The Reasons to Vote Accept
Criticism of the current strategic model
What’s next?
Click the ‘+’ sign in each section to expand and navigate the discussion.
The offer
The offer has been making headlines stating a 22% on average pay rise for members over 2 years. However, this is an oversimplification. The offer can be separated into eight parts.
Pay items
The already implemented pay rise of 2023-2024 of 6% + £1,250 (consolidated, worth 8-10.8% dependent on grade, skewed to favour lower nodal points). This is highly unlikely to change as a result of the member vote.
The addition of 4.05% on 2023-2024 pay, with backpay for any member who was on a 2016, 2002 or mirror resident doctor contract during this period, applied from April 2023 to April 2024.
The Doctors and Dentists Review Body (DDRB) advised pay increase for April 2024-April 2025 of 6% + £1,000 (consolidated, worth 7-9% dependent on grade, again skewed to favour lower nodal points). The DDRB advice is only a recommendation, but this government has committed to implementing it. Whilst the Government might have withheld some or all of this money if the RDC had not put the offer to members, it is highly unlikely to change as a result of member vote now that acceptance of the recommendation has been announced.
The application of the above pay increases will apply to locally employed doctors who make up 15% of the resident doctor membership, and be fully funded by central government.
The pay increase comes from new investment from the government, rather than cuts to NHS services – this is a major benefit and has ‘Barnett’ implications. Barnett is the mechanism by which the devolved nations' health budgets are increased. The deal would increase the money available to devolved governments to increase the pay for their resident doctors, including those resident doctors currently in dispute.
Non-pay items
Commitments to review training numbers and rotational training, aiming to correct bottlenecks in training, create jobs for increased medical student cohorts and reduce the burden of rotational training. These commitments, whilst on major issues, have little detail, nor time frame attached to them.
Reform of the exception reporting system to remove the need for approval by educational or clinical supervisors. Instead, responsibility to approve payment and/or TOIL will lie with HR, and exception reports relating to 2 hours or less will be paid without argument about the doctor’s decision.
An addition to the DDRB responsibilities – the DDRB will make recommendations which ensure doctors' wages in England are competitive. This is in the context of both international migration of doctors, and the Scottish deal which ensures at or above inflation pay rises for their resident doctors.
Concessions
If accepted, RDC must:
Terminate the current trade dispute (i.e. the pay campaign), with no specification of how long this must last, and no limitation on further industrial action.
Withdraw the current locum rate card; though, unlike consultants, there are no restrictions on the introduction of a new rate card at a later date and no limitations on rate cards for the devolved nations.
The pay deal is better than the offer the previous government made, under Victoria Atkins.
The previous offer did not apply to all nodal points, meaning some grades would have been left without a pay rise- this deal increases the wage of all residents.
The pay increase is 1.1% higher on average than what the previous government offered.
The back pay is new, and is significant, as is the inclusion of Locally Employed Doctors (LEDs) who are approximately 15% of junior doctors.
However, it is also not Full Pay Restoration.
-
Within our discussion, it became clear that the Broad Left agreed on the following:
This deal is not Pay Restoration.
Full Pay Restoration is a reasonable, affordable and winnable demand
The Pay Restoration campaign has been highly successful in consistently mobilising huge numbers of members.
The Pay Restoration campaign started with an effective and understandable strategy:
Creation of local WhatsApp groups for coordination,
Identification of local activists and pay campaigners,
Clear messaging internally about media training and engagement,
Frequent quick documents to the press and membership about the industrial action,
Use of multi-day full walk-out strikes.
The current RDC strategy to achieve Full Pay Restoration, however, has proven inadequate. There have been failures in:
Support of local organising and activity alongside, in some instances, active discouragement.
Strike planning, with limited variation, escalation and coordination
Negotiation strategy and transparency, such as backtracking on open negotiations.
Communication and messaging with grassroots members on the progression of negotiations.
This deal does not commit the English government to Pay Restoration. With this deal, resident doctors are still paid 20.8% less in real terms than 2008 levels by RPI.
The Broad Left believes that Full Pay Restoration is possible, and something we have pushed the BMA to fight for.
The disagreement is nuanced and based on differing thoughts on which tactic is the most likely to achieve Pay Restoration.
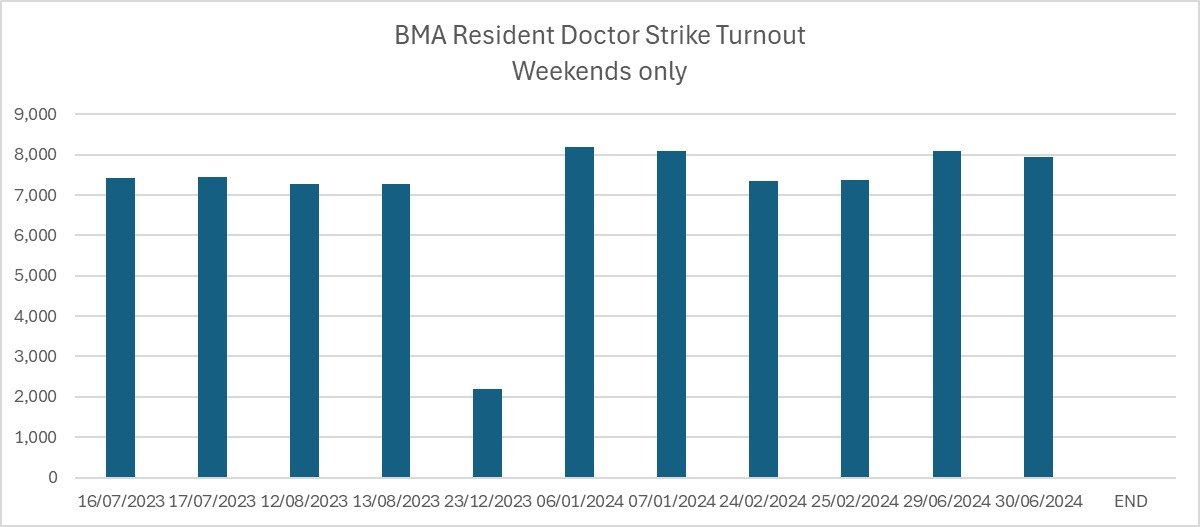

Data from NHS England shows strike turnout is high and consistent (data).
-
Some in the Broad Left believe that we should reject the offer. They feel we should push for a commitment to Full Pay Restoration over time from the UK government and/or a higher pay offer for this year. If this cannot be achieved by negotiation, then there will need to be escalated action, alongside potential coordination with other unions.
Others in the Broad Left believe we should accept the offer, banking the back-dated pay and using the nine months available before the next DDRB report to re-engage activists, solve some of the strategic problems in the campaign, and allow colleagues to save up money and advance training needs. Then, if the DDRB recommendations or the Government’s subsequent pay awards fail to represent significant ongoing progress towards Pay Restoration, we will be in a better position to take further industrial action.
The Broad Left has continued enthusiasm for the utilisation of industrial action for winning Pay Restoration, which we believe we can win. Both strategies require the re-mobilisation of doctors into rank-and-file activity, which will put pressure on DDRB to continue recommending above-inflation pay rises to doctors, and on the Government to accept this.
Below we will break down the arguments from both sides.
The Reasons to Vote Reject
-
There is a crucial concession in this offer: ending the dispute. Our formal dispute started in February 2023, after three years of campaigning from the grassroots to fight for Full Pay Restoration. This deal, if taken, will end our dispute whilst leaving resident doctors paid 20.8% less in real terms than those at their same grade in 2008. The offer, in fact, only takes our payback to 2021 levels. Accepting this deal means we accept not moving the needle - only being compensated for the economic downturn post covid. Doctors in 2021 were not paid enough, struggling to afford housing, exams and Royal College fees, and the same applies now.
This offer is not good enough, and on a very basic level if you think that doctors deserve Full Pay Restoration you shouldn’t vote to end the dispute for an offer that leaves us with the same level of pay cut that we were facing when we started.
Right now, our strike turnout is high and stable.
We have demonstrated that striking is safe for patients.
It is true that the current offer is higher than those received by other public sector unions and includes back pay. That is not a reason to accept; rather it is an indictment of the poor industrial strategy of other groups within the labour movement. Our offer has been made in response to the significant impact of our strike action. Official NHSE figures (included below) indicate that our strike participation rate is consistently high, surpassing that of any other public sector union. Weekend strike turnout is gradually increasing. Additionally, our ballot turnout remains higher than that of the RMT London Underground and is comparable to the RMT Overground turnouts.
The campaign for Full Pay Restoration still has significant momentum, despite talk of fatigue; burnout; poor messaging from RDC (e.g. the purpose of strikes is negotiations rather than winning); the removal of 'pay campaign activists' from and stagnation of workplace WhatsApp groups.
Picket line and rally turnout have fallen dramatically, but this creates a false impression of member disinterest in trade union activity. The data shows that strike turnout is holding up. We believe that pickets and protests have been organised as media backdrops, which means many feel they are a waste of time, without enough impact on the campaign to justify travelling to. This is not a picture of weakening resolve but of members choosing not to do things they perceive to have limited purpose.
Why is our action significant and consistent? Striking offers practical benefits for doctors.
We work 48 hours per week, on average, in work which we are often alienated from, looking after patients for only a few days at a time. Treated as disposable rota-fodder, there are few emotional draws to keep us at work. Striking provides the time which we have been robbed of within our rotas: to rest, spend time with family or engage in personal activities. The financial impact of striking, e.g. a 9.8% pay reduction for participating in three strike days per month, as part of a 5-day strike, is cost-efficient compared to the financial impact of working Less Than Full Time (LTFT i.e. less than 48 hours/week). Moreover, doctors generally do not need to extend their training due to striking, making it a financially efficient option.
The high and stable turnout for strike action, despite limited workplace organising from RDC, indicates that doctors are finding value in participating in strikes.
If we accept the deal we will waste the industrial power we currently hold. It will shift the narrative from a clear focus on reversing a large pay cut to a more complex and less compelling message of wanting more after a 22% pay award, which could make it harder to achieve and maintain strike participation in any future actions.
Other unions, such as the UCU, have experienced member disengagement and strike attrition in new disputes after ending previous disputes without achieving their goals. In contrast, the RMT maintains momentum by not ending disputes when the offer is inadequate. In 2016, the BMA ended the contract dispute blaming it on waning enthusiasm and predicted low strike participation, which led to member anger from those who had voted to reject the contract offer. Trapped in complex and confidential contract negotiations thereafter, the BMA failed to “rebuild”, and we have struggled to regain strength in the years since.
-
It takes time for the grassroots to effect change in the BMA.
The current campaign began in early 2020 when a group of doctors, including members of the Broad Left, attempted to join forces with nurses to advocate for a 15% pay rise for all NHS workers, reflecting the extent of pay cuts at that time.
In Autumn 2020, BMA grass-roots members passed a policy to survey the wider membership for potential actions, including industrial action, against repeated below-inflation pay awards.
In Spring 2021, Junior (now Resident) Doctors passed a policy cementing a goal of a 15% pay rise, joining the NHSPay15 campaign.
Despite the work of rank-and-file doctors and these policy changes in 2020 and 2021, RDC (then JDC) did not act on the mandate and took steps to undermine it, including surveying members with biased questions (a maximum demand of >5%) to suggest that most did not support a 15% pay rise.
During this period, grassroots doctors continued to push for Full Pay Restoration. This included workplace organising, the formation of Medics4PayRestoration and then later the formation of DoctorsVote. This helped shift the perception of Full Pay Restoration from unrealistic to reasonable and achievable. Candidates aligned with DoctorsVote, Broad Left or both took 26 of the 69 Council seats in the Spring elections in 2022.
We won policy in favour of Full Pay Restoration, and seeking a mandate for industrial action to win it, at the Junior/Resident Doctors Conference and the following BMA ARM in the Spring and Summer of 2022. By the time the RDC co-chairs took office in Autumn 2022, much of the groundwork for the pay campaign had already been laid by local activists.
Several years of rank-and-file agitation will need to be re-done if the deal is accepted, and perhaps on harder ground, given that we will be asking people to revisit a decision they made to accept and end the dispute.
-
Whilst our momentum is sufficient to continue, there is a question of how much further our current strategy can advance our pay deal. Whilst we are likely to achieve incremental changes to the current offer with the continuation of the current strategy, Pay Restoration would require organising industrial action that is so disruptive that it becomes less costly for the government to grant the Pay Restoration than to endure the disruption.
The BMA has estimated the cost of Full Pay Restoration for resident doctors at around £1 billion per year, while the government estimates it at approximately £2 billion. The new Labour government has acknowledged that the cost of ongoing strikes exceeds the cost of their current offer - this supports the notion that we can make further incremental improvements to this offer through the threat of further strike action.
However, both of those estimates are flawed - they view the current situation in a vacuum. Trade unionism is contagious. Giving us FPR will inspire action in other public sector workers, such as NHS staff, teachers, and civil servants, to demand similar Pay Restoration. The government has previously stated that the cost of Full Pay Restoration for all public sector workers could be around £28 billion per year, a figure that may now exceed £30 billion annually if matched to inflation. To achieve Full Pay Restoration for us, the campaign would need to generate enough disruption to match not only the upfront cost of our deal but the cost of every other dispute which would follow. Our current strategy is not generating such a cost. Despite high and stable strike turnout without significant room for improvement, hospitals are becoming more effective at mitigating the impact of strikes, cancelling fewer appointments, leading to reduced disruption.
To counter this, and to cause the cost of disruption required, we will need to coordinate with other unions.
At the start of the campaign, there were suggestions of an indefinite all-out strike of doctors, but this is unlikely to work. Doctors are not in a position to arrange collective meal provision and rent/mortgage strikes to survive a long period without any wages and would be unable to achieve career progression.
We are unlikely to get much further on our own. We will need to start collaborating with other unions and NHS staff to prevent actions that undermine strike efforts, such as arranging alternative cover or reporting payroll deductions for striking workers.
The most significant untapped source of power, however, lies in mobilising other public sector workers to organise high-participation industrial action. Highlighting the pay cuts faced by these workers, sharing strategies used to improve the BMA bureaucracy, and teaching effective strike organisation could lead to coordinated public sector strike action, increasing the overall disruption.
Rejecting this deal helps us in mobilising other trade unions, as it will be a public refusal to accept less than what we are worth, and a show to the other unions that they can and should fight for better than the 5% they have been offered. Accepting stalls our campaign, making it difficult to convince other workers to fight for better.
-
The RDC’s current suggestion to "bank and rebuild", or "bank and launch a new dispute soon", is a common suggestion across the labour movement when an inadequate pay offer is put forward. What follows is an inevitable quieting of activities, as those unions are no longer in active dispute.
So far, RDC has not provided any concrete steps for what will happen after the offer is accepted, and there is no clear plan to achieve Full Pay Restoration.
Instead, having previously removed some local reps from workplace WhatsApp groups and centralised power, RDC is now suggesting the next steps are to empower local reps. This comes after the public rejection of radical empowering reforms, such as establishing workplace-based divisions (branches), including by some current RDC members worried it would reduce their electoral power.
Despite some early reforms such as publishing Council minutes, and power on the Organisation Committee and Council, DoctorsVote has not significantly changed the BMA or RDC structures or processes. At times they have lacked majority or ability to build consensus, and at other times they have been a conservative force. This means the BMA and RDC are not equipped to “rebuild” the effective campaign that has brought us this far.
This has occurred partly because many of the original founders of DoctorsVote, who wrote and implemented the original rank-and-file strategy, are no longer involved. They have been replaced by more ‘moderate’ voices, and their original DoctorsVote posts with clear and public strategies have been mostly removed from reddit. The original website has also been taken down, and the Discord server where lots of grassroots work took place has been mostly inactive since 2022. These actions have induced amnesia about the significant and good work the large and open DoctorsVote organisation took as grass roots members to agitate activity and get us to strike action.
This amnesia allows DoctorsVote leaders within RDC to claim that their work within the BMA structures is responsible for the pay campaign, whilst undermining the tactics which gained us the momentum we currently enjoy.
Unless there is a clear, transparent, laid-out plan to achieve remobilisation on the bank and rebuild strategy, there can be no “faith” that the current RDC plans to continue the campaign once the deal has been accepted.
-
The parts of the offer affected by our vote amount to only an average of 4.05% for 23/24, and 4.4% for 24/25, and some weakly worded commitments. The Government’s acceptance of all DDRB recommendations for 2024/25, means that members will receive 7-9% this year even if the offer is rejected.
Consultants in England rejected their first offer, and, in doing so, exerted significant pressure on the Tory Government to immediately propose a better deal. We could achieve something similar if we voted to reject and re-entered negotiations. Even a commitment to FPR, which admittedly holds little water, would fuel doctors to take further action if betrayed, as we saw in Wales.
In contrast, accepting the deal would give politicians, the public and the media the appearance of a settled matter. This will impact our ability to undertake further industrial action on FPR in the future.
If we accept the current offer there will be nothing to rally against, only a muddied message that we should fight for more.
{kind=link}
The Reasons to Vote Accept
-
This deal adds to any wage earned between April 2023 and April 2024, and will likely be the last easy opportunity to add anything to the 23/24 pay award. This creates significant back pay, which would go not only to those currently practising as Resident Doctors but also to those who have completed training or left England. It is worth noting that most of the pay uplifts we have won so far have come from DDRB and not direct negotiations. Whilst more welcome than the real-terms cuts of the past, DDRB pay awards are not retrospective and give no opportunity for backdating.
This is also the first offer to include funded pay rises for LEDs. Locally Employed Doctors, such as clinical fellows, are those resident doctors employed directly by trusts on non-standard contracts, mirroring the 2002 or 2016 contract. Clinical fellows and other non-standard roles make up ~15% of us and are disproportionately IMGs or people affected by training bottlenecks. Central funding for LED pay reduces the need for doctors to negotiate locally for pay awards. This will reduce further expansion in the ethnicity pay gap and the impact of bottlenecks on long-term pay and pensions for those stuck. It has the potential to increase BMA membership amongst IMGs. It also reduces the risk of LEDs breaking strikes in the future, either in their job role or by taking locums.
The offer is funded with new money from the Treasury, which means our pay is not funded from NHS cuts, and creates Barnett consequentials (new money for the devolved nations). This will create negotiating power for our colleagues in Northern Ireland, Scotland and Wales. Their advances towards Pay Restoration will then further benefit English progress.
Commitments to Pay Restoration mean very little. Welsh Labour was comfortable with reneging on its commitment to Full Pay Restoration. The addition of a commitment to Pay Restoration to this offer would mean nothing in the context of a government advocating for further cuts and austerity. Funded pay rises are needed, and this offer takes us ⅓ of the way.
-
Our current industrial action is sustainable and strong.
Due to rota systems and low staffing, resident doctors lack consistent colleagues to form relationships with and have little patient continuity, alienating us from emotional links to our work. Many are burnt out. Doctors therefore enjoy the break from 48-hour weeks that enables time with family and friends we may not otherwise get. The financial and training impacts of striking are less than working part-time. Doctors lose only 1/365th of annual pay per strike day and do not generally have to extend training.
We could continue this current model of industrial action, potentially indefinitely.
However, all is not rosy. To win Pay Restoration, the cost of action - politically and financially - has to be more than the cost of resolution.
Politically, our offer came as the new government announced massive cuts to other services. They have staked out their economic approach of “nothing unfunded”. To shift this government to agree to Full Pay Restoration over time is to ask them to commit to paying above unknown rates of inflation and therefore commit an unknown amount of funding, contravening their current fiscal strategy. To shift them to pay up immediately would push them into tax rises or other cuts they are committed to avoiding. The government will strongly prefer to use the cover of the “independent” pay review bodies to avoid making politically difficult decisions and seek to wait us out until 2025.
We do not accept that the government's economic austerity policies are fixed, nor necessary, but winning more will require undermining those policies.
We would have to cause such disruption that ending the action by announcing an even higher pay offer would be politically advantageous, and economically preferential, for the government in comparison to the criticism they would receive for doing so in the context of such issues as the winter fuel allowance changes. Our current action is not doing that.
Financially, Pay Restoration has been estimated as £1-2bn for residents, but given that effective trade unionism is contagious, the cost would be over £28bn for the wider public sector. Our action is not generating even the in-year costs of Pay Restoration for doctors.
Trusts are progressively getting better at organising non-emergency work around the strike action, reducing their impact and cost. We are also seeing increasing numbers of residents breaking the strike for locum rates, which are not as high as Consultant or SAS Rate Card rates, again reducing the cost of the strikes. There have also been small, but progressive, reductions in ballot turnout and reduced engagement in the campaign.
-
If the offer is rejected, even with a renewed strike mandate, sustained strike action at the current level from residents alone is unlikely to get us much further. The DDRB may award another above-inflation pay increase next year, but with no power to backdate and no associated policy improvements - those would be lost.
Escalations such as permanent out-of-hours strikes may help us win more, but not Full Pay Restoration, at the cost of significant intra-professional difficulties with our supervisors forced to cover. Small losses of salary from the current model of action are recoverable with locum shifts, but add more days and the current stable high turn-out may suffer as more become financially unable to take part. All-out strike action has been touted but is unrealistic for doctors who want career progression and have no capacity for collective meal provision and rent/mortgage strikes. The difficulties with these forms of escalation, and the likely limited additional costs they would impose on the NHS and government, may mean that some doctors incur significant losses without moving the dial in negotiations.
Significant further action without significant further gains in negotiations or from DDRB pay awards is a recipe for killing the action, slowly at first, but with eventual collapse.
Strike and activist fatigue is not inevitable. However, strike and activist maintenance does require clear progress towards goals, transparency and involvement. Acceptance of the offer demonstrates that we can take safe, consistent and impactful industrial action and achieve a 22.4% pay increase, far more than other public sector workers who have not taken action. Organisation and mobilisation, especially if we can make a clear pay claim and strategy for next year, is definitely possible.
In the case of rejection, RDC is unlikely to achieve significantly more from the current industrial action strategy. Cultural and structural changes needed to maintain escalated activity would take significant work and reflection. It would be optimistic to expect that change in the short time frame between referendum results and a re-ballot.
-
The only way to create costs of >£28bn, pushing the government towards Pay Restoration, is to coordinate action with other unions.
We are currently the only major union in dispute with the government. There are 14 unions in the NHS alone, and several more across the public sector. Successful efforts to coordinate with other unions so far have been limited: only one day with radiographers, and one day overlapping with teachers and civil servants. The biggest NHS unions, Unison and RCN, have been in national pay disputes recently which have collapsed. Unison’s Health Service Group Executive has moved to a more moderate position following recent elections. The RCN pushed out many activists who opposed the recommendation of the 5% offer in 2023. Whilst this government has announced multiple public sector pay deals simultaneously, there is little effort from other union leaders, and no clear political pressure from rank-and-file activists in other unions, for coordination around pay demands. Some unions are not voting at all. Politically, very few unions’ leaderships are radical and up for the kinds of sustained industrial action we have been using, let alone coordinated action on the scale we would require, especially under the new Labour government.
It took BMA members and activists like us several years to push the BMA into a proactive position on Pay Restoration, we cannot expect activists in other unions with more complex structures and competing professional interests to manage to do the same in a matter of weeks. Whilst we should continue seeking coordination and encouraging other trade unionists to organise in their unions for better pay demands, we must be realistic about what is achievable in the remainder of 2024. Sustained coordinated strike action with other unions is probably not realistic, and cannot be relied upon to get us a better deal.
In addition, RDC has made the exceptionalism of doctors a key feature of our campaign. Arguments that we have fared much worse than other groups of workers (and therefore deserve more) and that we are unique in either our profession or our trade unionism, encourage separation from other workers in both our minds and theirs, not collaboration. A motion to join the TUC was defeated at ARM 2023 with coordinated DoctorsVote opposition, and doctors’ engagement with the rest of the labour movement is slim.
In the NHS, the inter-professional and inter-grade conflict between residents and other groups is fostered by rotation and poor treatment, further reducing the chances of joint working at the workplace level. Even coordination with Consultants was difficult due to the need for a “Christmas Day cover” approach, and many resident doctors were disaffected by this.
GPs are swinging into collective action, however, much of this will be technical changes such as withdrawal from data sharing agreements and medicines optimisation. Whilst strike action from GPs may come in the future, this is not likely to be imminent. It does not offer much chance of coordination with residents.
Our isolation will take time to reverse in both the minds of doctors and other groups of workers.
-
The question is not whether the deal is amazing - it is not. There are definite benefits, but it is not Pay Restoration.
To achieve Full Pay Restoration, we need to change our strategy. We might make bigger steps towards Pay Restoration with escalated action but decreased engagement and political circumstances are against us. Coordination is not coming quickly enough for a complete victory. In the absence of either of these, any further significant improvements in pay are likely to come at or around the next DDRB announcement. The question is, what's the best strategic move to ensure that further pay rises are won and action is successful? And what is in our best interests in the meantime?
If we accept the deal, we put money into doctors’ pockets, allow recovery of training time and demonstrate the success of strike action compared to colleagues elsewhere in the public sector. We give ourselves time to further build the strike fund - new in 2022 - through the allocation of a 1% increase to member subs fees. This will support those beginning to struggle financially with strikes to participate in the action.
We can re-recruit, train and educate reps, ensuring we maintain both our internal coherence across rotations and start to turn outwards to the rest of the labour movement. We ensure our plans for further action are solid, with maximum accountability between members and national representatives. We give ourselves time to make the kinds of arguments that pushed the BMA into a proactive pay campaign in other unions.
We may even benefit from changes to trade union legislation.
With this deal, we have achieved 22.4% and a DDRB change from 18 months of IA, without selling out the principle of Pay Restoration. With a strong demand for DDRB 2025 and the government’s response to it, we could have a clear trigger point for formal re-engagement in a dispute and a demonstration of how effective strike action can be. Both the DDRB and government will be keen to avoid us remobilising as we have shown we can.
We should not reject the pay offer solely on the basis that it does not promise Pay Restoration - we have seen such promises turn to mist in Wales. Rejection of the pay offer because you feel we can mobilise now and get a better immediate pay rise is a fair position, but there are valid questions on how possible it will be to make the changes to our strategy needed to achieve this in such a short timeframe.
Rejecting the offer requires a belief that doctors, who whilst consistently striking are increasingly disengaged from the campaign, will rapidly: change their minds about coordination with other workers; force RDC to change tack; convince other workers to take action and create pressure for other unions to change their strategies.
We believe accepting this offer is the best tactical decision to achieve Full Pay Restoration and union transformation. We still have a lot of work to do to rapidly organise our members and those in other unions, keeping them engaged and in ownership of the industrial action. All in the Broad Left who vote in favour of the offer will fight for the action required to win better, we think banking a partial win and giving ourselves time to do the work is vital.
Criticism of the current strategic model
Regardless of how members vote, the Broad Left has also identified what it believes to be key issues with the current strategic model. We believe the following areas need interrogation and assessment to ensure the mobilisation of members and the acquisition of Full Pay Restoration.
-
This action was born at the grassroots from 2020 onwards, and was galvanised by the incredible formation, growth and electoral success of DoctorsVote. With it, the membership has mobilised to strike frequently. However, after winning the vast majority of RDC seats at the election, DoctorsVote elected members have overseen consolidation of power centrally into RDC, reducing the involvement of local activists in decision-making, whilst instructing those same activists to undertake significant work.
As past leadership decisions can show us, even good workplace representatives are changed when elected to national roles. This is not a personal failing but rather a structural problem with trade union bureaucracy. We partially protect ourselves from this in the BMA by having part-time representatives, who are also working doctors. However, the rank-and-file members must have genuine power and accountability to prevent paternalistic approaches, or selling out, from elected leaders. Centralisation of control has benefits, such as excellent media discipline, and this strategy has delivered us the current deal. However, it also has significant drawbacks.
Mapping, charting and organising for ballot success and strike action takes energy from individual activists in every workplace. At the start of the industrial action, local activists ran organised ward walks and built networks in hospitals, both in person and via WhatsApp groups. Reps organised local pickets with sometimes massive participation and engagement from members. Picketing and strike-day activities have since been deprioritised by RDC members, without replacement foci, and that has led to reduced involvement of those local reps and activists. Input into industrial strategy has also been largely rejected by those outside of established factions within RDC. It’s not uncommon for local activists to feel unable to influence RDC unless they become members of DoctorsVote, which has become cliquey in places. Without activities to galvanise around, concrete goals to focus on, or leaders willing to seek out and listen to their points of view, practical engagement from activists within the wider membership has fallen.
RDC members also set up local WhatsApps across the country, specific to each trust, at the start of the action. This concept was a great idea; ensuring that whilst resident doctors may rotate and find themselves separated by rota and distance, they could still communicate on the issues which unify them, and then organise collectively. WhatsApp strike groups were a useful tool during the first rounds of industrial action. However, alongside feeling adrift and under-informed, local activists and representatives have been undermined in their activities through restrictions on the use of these WhatsApp groups. In some places active local organisers have been removed from the groups, prohibited from organising strike events and chastised for charting members’ feelings whilst picketing. Aggressive policing and limitation of discussion to only strike-related topics have hindered activists’ ability to map and chart memberships of these groups for each workplace, especially around strike participation. This approach has also ensured limited to no discussion occurs within said groups during RDC’s prolonged periods of closed negotiation.
The failure by RDC to galvanise local action within individual WhatsApp groups, and coordinate doctors in changing/leaving groups once they moved to a new region/workplace, has turned a good idea of local large peer messaging groups for organisation into dormant broadcast pages muted and left forgotten by many colleagues. Now, all picket instructions come from the top (RDC) and even ‘regional’ picket lines show poor participation. The centrally organised national rally during the 2024 election produced a poorer turnout than the early DoctorsVote demonstration organised in early 2022, despite the provision of funded coach transport. This can be taken as evidence that engagement has fallen.
The disengagement between the members of RDC and the membership puts us at risk of repeating some of the same mistakes as we saw in 2016. Whether this deal passes or not, there needs to be significant work on empowering people locally.
-
The largest improvements to pay have not come from the negotiation room, but from the DDRB. The DDRB’s recommendation to increase our pay for 2024/2025 would not have been as high without the industrial action. We know that the DDRB is not independent but a political instrument, and their reports mention the “industrial unrest” as a key reason for the above inflation recommendations. The Government is under no obligation to accept the DDRB’s advice, and previous governments have ignored recommendations, but both Conservative and Labour governments have accepted recommendations during our dispute. Industrial action has improved our pay, though not yet back to 2008 levels, through pressure on the DDRB. The “bank and rebuild” strategy still requires the DDRB as a trigger point, when direct negotiations would put more power in doctors’ hands.
The RDC members in the negotiation room, however, have not adequately demonstrated their ability to argue for Pay Restoration directly with the government. This is, in part, due to a lack of transparency and communication about those negotiations and our leverage.
-
Lack of open (or high transparency, high participation) negotiations
There have been no open negotiations. At the start of our dispute, RDC had agreed to transparency and accountability to members for any forthcoming negotiations. This was to engage with our members at the grassroots level and potentially prevent the events of 2016. However, members have been kept in the dark about the negotiations, who our RDC negotiators were and how they have been acting on members’ behalf. None of these details have been communicated to members, nor whether the Government has offered any other deals other than a small percentage rise. Despite early moves from Broad Left and some DoctorsVote members, including those on the BMA Trade Disputes Preparedness Group (a group of staff and BMA Council members), to advocate for open negotiations, this was rapidly abandoned.
Open bargaining uses radical transparency, elected negotiators and larger teams to create pressure on the opposing side. This reduces the ability of the opposition to split the negotiating team from members or put forward a bad offer whilst everyone is watching, naturally has the pulse of members and allows wide scrutiny when core negotiating team members are fatigued. It has been used in trade union negotiations in Europe and the USA, and can be read about here, or watch here.
Further, despite a move to publish minutes from Council, the push from DoctorsVote to record all votes at conferences, and recording of votes in the minutes for RDC, no minutes of RDC have been published during the dispute.
Lack of information about strike participation
Members have not been told about engagement with strikes and the impact on negotiations. RDC have been collecting strike participation data via “dipstick poll” and via the data from NHS England. Some trusts have detailed data, but it is unclear if this has been collected or analysed systematically. None of this information has been shared with reps and activists on the ground who would be able to target problem areas, know where turnout has been consistent, gauge appetite for escalation or advocate for control of any changes to strategy. Our analysis is based on NHSE data, which is partial and poor in places, and has no consistent denominator.
-
We have also seen a rise in issues beyond pay; unchecked expansion of MAP roles without official scopes of practice, worsening bottlenecks, limited job opportunities for GP trainees completing training, training opportunities being lost, and many other issues with significant impact on the membership. However, members have very little idea of the work of the BMA and RDC on these issues. The anaemic RDC ARM 2024 report is a damning indictment of how RDCs current activities have halted improvements to terms and conditions in the aid of the pay campaign - see the document at https://www.bma.org.uk/what-we-do/annual-representative-meeting/arm-reports-for-2024
Alongside this, we have seen a reduction in the diversity of elected representatives across the BMA, and RDC is a prime example of this. For the past 2 years, RDC has had reduced diversity amongst members from some protected characteristics, including women and Black members. Without representation of those members, RDC runs the risk of lacking the diversity of thought required to assess and support issues within differing communities.
What’s next?
Some broad left members will organise to reject the deal. Some will be advocating for acceptance. Regardless of the outcome, we will continue to fight for Full Pay Restoration, transparency in the union, and a better life for our members and our patients. Many of the required actions following the vote will be the same, only varying in terms of timeframe.
The Broad Left will seek to facilitate discussions and ensure that regardless of how members vote, we do so with insight and in high numbers.
In the event of a no vote
In the immediate aftermath of the vote, we will need to re-mobilise and rebuild. We need to organise to deliver a successful re-ballot and good engagement with strike action thereafter.
Rebuild local structures within the months of August and September, relying on changeover in August.
From October, immediately after the pay deal vote, the priority must be to re-ballot members. Data cleansing should require limited time due to the referendum, but the actual postal ballot will take 1-2 months. This period will offer immediate opportunities for meeting with the Government for further negotiations and exerting pressure via imminent renewal of the industrial action mandate.
We must immediately restart rank and file organising, including cross-profession. Face-to-face work will be necessary to gauge appetite for various types of action, their readiness to strike and escalate action, and, if necessary, galvanise those members. We need information on members’ ability to strike against constraints on their financial resources, professional commitments, training opportunities, and so on.
After achieving another successful mandate, we must ensure the strike action is effective and successful through rank-and-file organisation across the union.
In the event of a yes vote
In the immediate aftermath of the vote we will need to:
Emphasise that this is a provisional victory in the fight for Full Pay Restoration, with 18 months’ worth of action, roughly 9% of members’ wages lost, leading to a 22% pay award (in comparison to 4 years of 2% awards).
Push RDC to make clear demands of the government regarding the 2025 pay award, ready to trigger a further formal dispute.
Advocate for RDC to adopt a public strategy of escalation and coordination with other unions, and work with other activists in our hospitals across unions on a rank-and-file network basis.
Rebuild local structures and organising across the next year
Emphasise the need for members to prepare for remobilisation and a new ballot for strike action for Pay Restoration at the next pay award (~April 2025), and be prepared to agitate on the lateness of the DDRB recommendation should the recommendation not be made public within the month of April.
Regardless of Result
We will need to:
Seek new activists across the union, including those angry at the deal, to take up active roles as LNC reps and local organisers; we need to get more members into BMA training and encourage standing in elections for representative roles.
Develop a strong pay-militant RDC leadership which is ready to prompt new negotiations with the government and coordinate the next ballot for industrial action to continue the fight.
Push for transparency and improved communications by RDC, via the publication of RDC minutes, and immediate member-wide updates on the full extent of negotiation discussions after every meeting
Seek fundamental change in the negotiation strategy by RDC.
Push RDC and members for mutual active engagement in industrial action strategy. We must demand that RDC actively discuss with members what they can and will do for FPR.
Push RDC to meet with other unions to discuss joint action where possible to amplify and escalate the potential or actual impact on service provision and the Government.
Create closer relationships with other unions in our workplaces, to achieve coordinated action in the future. This includes attending grassroots activist meetings, joining rank-and-file networks like NHS Workers Say No, and encouraging them to use the tactics established in our pay campaign to enact swift and effective democratic change in their own groups.
Revise WhatsApp groups for coordination by local activists.
Build strategies for developing other disputes on issues beyond pay such as MAP role scope and substitution, improving terms and conditions, expanding training numbers and reducing costs in training.
Seek accountability for all of the work of RDC over the last two years, including on issues beyond pay
Educate the membership on fundamental trade union activity, to ensure that the next fight, whenever it is, is not reliant on the Broad Left, DoctorsVote or any other currently active organisational group.